Like the hip, knee pain can have causes that aren’t due to underlying disease. Research suggests that thorough clinical examination is generally very reliable at ruling out various knee pathologies, including internal derangement disorders. With these disorders excluded, a more functional approach to the pain condition can begin. As a clinician we start by asking ourselves these questions:
- Has there been any damage to the meniscus or cruciate ligaments?
- Is the knee stable?
- What is the primary pain generator?
- Is there joint dysfunction or any soft tissue problems?
- Are there any other contributing/predisposing factors?
From this point we start to map out a treatment and rehabilitation program to fix the structural issues while improving the motor programming of the lower extremity. We know that knee pain stinks and that it is annoying. We know it can impair performance and can be life altering at times. It is our goal at [Core] to quickly and correctly identify these issues to get you back to health.
Anterior knee pain, also known as jumper’s knee, runner’s knee, or patellofemoral tendonitis, is easily identified by pain around the front of the knee, specifically, just below the patella (kneecap) or behind it. The good news is that you can do something about it; the bad news is that it’s usually caused by overuse within a dysfunctional movement pattern. That means that rest and re-establishing proper loading and movement through your knee and hip is one of the best ways to alleviate the pain. We realize sometimes taking weeks off isn’t an option, so our goal is to alleviate some pain through proper training.
To understand how to alleviate some pain, we need to understand some anatomy. The patella is a free floating bone on the front of the knee that is held in place by two tendons: the Patellar tendon and the quadriceps tendon. The Patellar tendon connects the patella to the tibia while the quadricep tendon connects the patella to the quad. The patella acts as a sort of fulcrum for the femur and the tibia, increasing force of the quad.
Substantial loads are placed on the patella; 2-3 times your bodyweight when walking and up to 5 times your bodyweight when running. Now imagine how much load is placed on the knees when jumping, especially in tall athletes. If their strength is inadequate and the knee and foot sit decentrated, stress will be placed on the tendons and ligaments (for example, the Patellar tendon). A lot of professionals will simply suggest strengthening the hips, but what does that really mean? Let’s look at the specifics. Weak hip abductors and extensors can lead to anterior knee pain. Specifically, that’s the glute med, glute min, and Tensor Fascia Latae. Think posterior chain here, or the musculature on your back side. This is generally paired with tight or overactive hip flexors and adductors. If you take one thing away from this, remember this: pain isn’t normal. Athletes with knee pain consistently have weak/underactive butts and hamstrings and tight/overactive hip flexors and groins.
How do you test Glute strength and Hip flexor tightness?
 Hip extensor strength test: You can test glute strength by laying on a flat surface and raising one quad off the ground. Have a friend gently press down on your hamstring and attempt to resist them. Your goal is to resist as long as possible. If you are unable to resist some light pressure, you could have some glute weakness.
Hip extensor strength test: You can test glute strength by laying on a flat surface and raising one quad off the ground. Have a friend gently press down on your hamstring and attempt to resist them. Your goal is to resist as long as possible. If you are unable to resist some light pressure, you could have some glute weakness.
Thomas test: This is an easy way to check tightness of the hip flexors. Lay on a flat surface with your legs dangling off the end. Slowly bring your right knee to your chest and hold gently. If the left leg lifts off when you pull your right knee to your chest, then usually you have tight or overactive hip flexors.
Another reason athletes can suffer from Anterior knee pain is from abnormal tracking of the patella. This is oftentimes due to a neuromuscular issue. The picture here gives you an idea of a patella tracking abnormally.
How do you treat Anterior knee pain?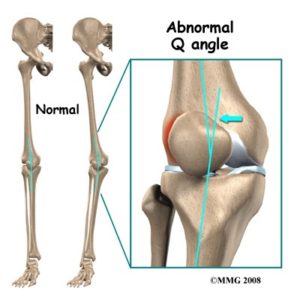
All joints have ideal positions. When a knee is sitting, let’s say, “out of alignment” or “decentrated” there will be pain due to the friction created by the movement of the patella. The ideal position is for the patella to be tracking in line with your middle toe and not really traveling too far in front of the foot. If you can fix this dysfunctional tracking, you can alleviate the anterior pain, almost instantly.
If you are reading this and have knee pain, take a look at your knee in the mirror, and see where your knee is sitting in relation to your toes. If you can’t tell, take a picture and send it over! We’ll be happy to help. Where it sits is a tell tale sign of where you have dysfunction.
Myofascial release
First, you need to do some type of myofascial release. I would suggest rolling on a lacrosse ball or a foam roller. This should be 30 seconds per spot, hold in the painful ones, concentrate on calves, hamstrings, and adductors. I would recommend staying to the edges of the IT band and not directly on the tendon, as it can irritate it. If this home therapy seems to be fruitless, then make an appointment in the office and we will apply Active Release Technique to the muscle adhesions to fix the muscle problems.
Mobility Work
Mobility work, often referred to as dynamic stretching, is a way of developing good motor programming while increasing the range of motion of joints and muscles. All athletes are different, but some key areas to address are adductors (groin) and hip flexors. You will generally know if your adductors are tight by performing a simple wide squat. Make sure you assess whether this is a chronic issue, or just some soreness due to a previous workout.
- Triplanar calf stretch 3 x 15 reps
- Adductor squat hold 2 x 30 second holds
- Adductor dynamic stretch 2 x 5 per side
- Reverse Nordic 2 X 15 reps
Posterior chain strengthening
Finally, you should incorporate some posterior chain exercises into your warmup exercises before running, cycling, or performing yard work. The primary goal of these exercises is to strengthen the glutes and posterior chain. Remember, these are great exercises to start retraining the glutes. The goal is to reduce pain and increase strength.
- Resisted Clam shell – 3 x 5 per leg
- Banded Glute Bridge – 2 x 10
- G-medius plank – 2 X 6 per leg
- Eccentric Single leg squat – 3 x 10 per leg
Core Retraining: The Bear
 The bear is an exercise that I have pulled from Dynamic Neuromuscular Stabilization (DNS). It is an incredible exercise to establish proper joint centration of the shoulders and hips, while being able to get your body into proper position within the spine. This position will also allow you to feel what intra-abdominal pressure is truly meant to feel like. It’s not just holding a deep breath, but actually setting your ribs on your hips, taking a deep breath down into your stomach with expansion not just forward through your rectus abdominus, but through your obliques. Truly feeling this pressure will change your world! Being able to properly center your shoulders and hips will directly carry over to better posture when running, sitting, and standing. I have seen significant changes in posture the instant an athlete can achieve the position on their own.
The bear is an exercise that I have pulled from Dynamic Neuromuscular Stabilization (DNS). It is an incredible exercise to establish proper joint centration of the shoulders and hips, while being able to get your body into proper position within the spine. This position will also allow you to feel what intra-abdominal pressure is truly meant to feel like. It’s not just holding a deep breath, but actually setting your ribs on your hips, taking a deep breath down into your stomach with expansion not just forward through your rectus abdominus, but through your obliques. Truly feeling this pressure will change your world! Being able to properly center your shoulders and hips will directly carry over to better posture when running, sitting, and standing. I have seen significant changes in posture the instant an athlete can achieve the position on their own.
Perform this important core stabilizing exercise by assuming the bear crawl position on all fours and breathe deep into your pelvis. Look to feel the breath and increased abdominal pressure deep in the pelvis and through the sides of the abdomen. Try holding this position through 10 slow breath cycles.
This article is not all encompassing on how to assess and deal with anterior knee pain. These are tools you can use to decrease pain and return you back to your normal routines. If you take one thing away, remember this: individuals with knee pain consistently show patterns of weak/underactive glutes and hamstrings and tight/overactive hip flexors and groins. Attacking these patterns with the right approach will quickly help you become healthier than you have ever been.

Daryl C. Rich, D.C., C.S.C.S.